Anticavity Dental Rinse
Biomimetic system for Guided Enamel Remineralization of early caries
– Professional product, for dental professionals only –
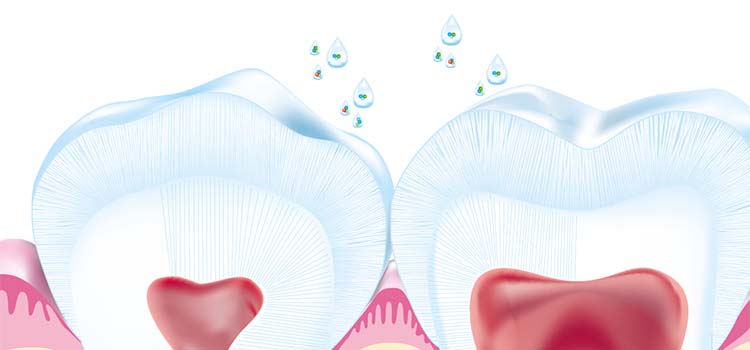
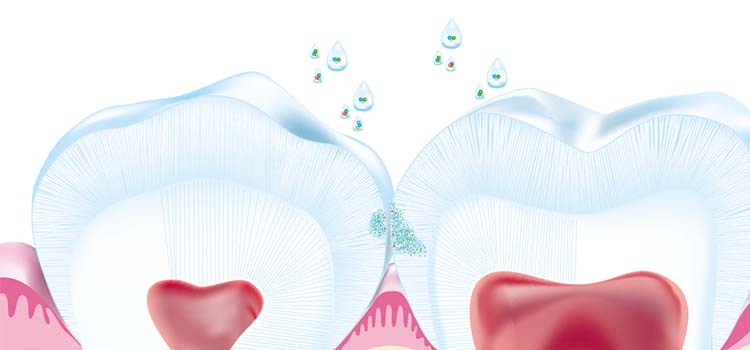
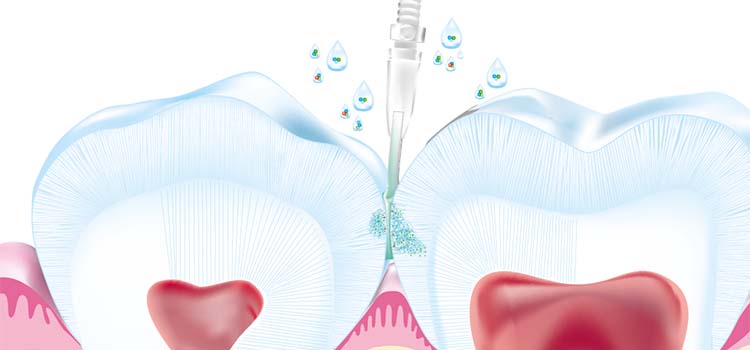
CURODONTTM Repair Fluoride Plus is a biomimetic, brush-on system that tackles early caries through Guided Enamel Remineralization.
Its patented formulation helps minerals diffuse into the tooth to remineralize and reharden the enamel, helping preserve the natural tooth structure.
Easy and fast application – Non-staining – Minimally invasive – For all surfaces – For all patients – One-time application.
1 box with 10 applicators can treat up to 30 lesions.
![]()
![]()
![]()
![]()
![]()
Box contains 10 units of ready-to-use applicators.
One applicator can treat 1-3 lesions per patient.
USE
In office
Sodium Fluoride, Water, Chlorhexidine diglucconate, Tromethamine, Trehalose Dihydrate, Oligopeptide-104, Hydroxypropyl Methylcellulose
USE
In office

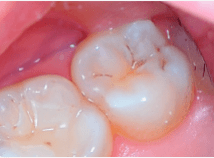
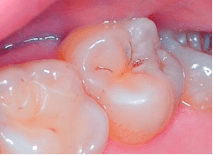
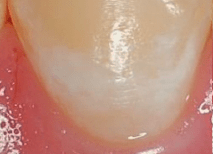
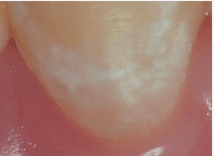
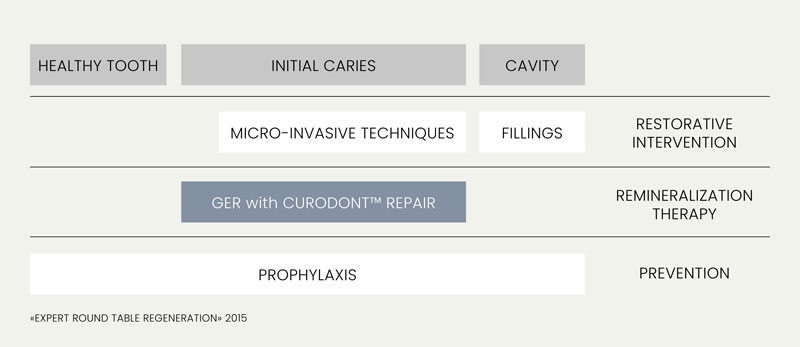
Guided Enamel Remineralization (GER) tackles initial carious lesions. GER bridges the gap between prevention and invasive restorative approaches. It enables effective therapy of initial caries and white spots through in-depth remineralization of the enamel, while still maintaining the integrity of the tooth.
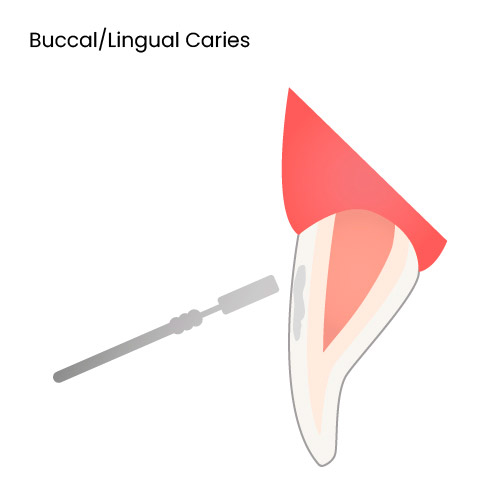
Smooth Surface
Application Video
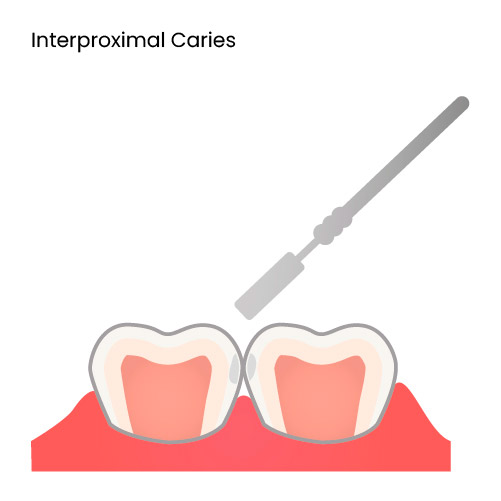
Interproximal Surface
Application Video
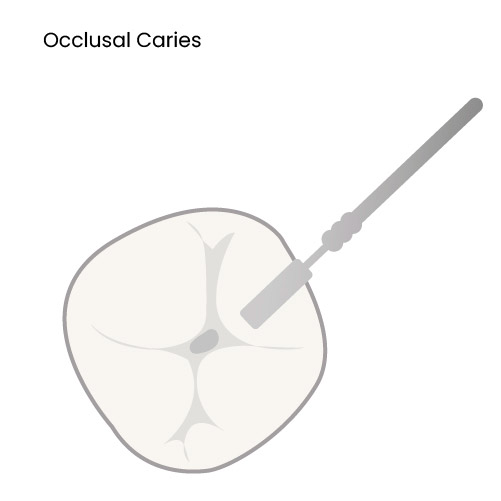
Occlusal Surface
Application Video
Ortho Case
Application Video
Alternatives to sodium hypochlorite include air polisher, prophy paste, pumice etc. as mechanical means of removal of organic content and the salivary pellicle. If these alternative methods are used, it is important to rinse the tooth thoroughly after this step.
The use of 2% sodium hypochlorite may be a more ‘thorough’ way to remove the salivary pellicle and organic matter.
Yes, the use of fluoride varnish or any other remineralizing paste is permitted after the use of CRFP. These agents act as suppliers of calcium, phosphate, and/or fluoride ions to the CRFP technology within early carious lesions (watch areas/white spot lesions), thus supporting the Guided Enamel Remineralization.
When using these agents, they must be applied at least 5 minutes after the application of CRFP in-office or after the appointment, at home.
An ideal complement to Curodont Repair Fluoride Plus is Curodont Protect. This anti-cavity dental gel can be applied once a day for one week (or until the tube is finished) on a lesion that has been treated in-office with Curodont Repair Fluoride Plus.
In the CRFP protocol, we suggest using unwaxed floss to effectively apply the phosphoric acid gel on proximal surfaces. There are two reasons for preferring unwaxed floss over waxed floss:
CRFP is a treatment for early caries. The CRFP technology works by enabling the diffusion of remineralizing ions into the body of early carious lesions (watch areas/white spot lesions). Thus, it is not an appropriate product to use on intact tooth surfaces.
Curodont Protect, an anti-cavity dental gel, would be an ideal product for caries prevention, including for patients at high caries risk.
Whitening toothpastes depend on different mechanisms to achieve the whitening effect. Many toothpastes depend on hydroxyapatite for whitening, in which case, there is absolutely no issue with using it right after a Curodont Repair Fluoride Plus treatment. The hydroxyapatite may assist in the remineralizing action of Repair.
However, even if the whitening toothpaste is peroxide-based, it may be used post-CRFP application. The peroxide content in whitening toothpastes is fairly minimal and the ‘brushing’ action ensures that the contact time of the agent with the CRFP technology within early lesions will also be quite low. Thus, the probability of peroxide from these toothpastes interfering with the action of CRFP is very low.
In most cases, except when caries involves the outer third of dentin while the lesion is still non-cavitated, we would not recommend using CRFP.
CRFP works by enabling the diffusion of remineralizing ions, such as Ca2+ and F-, in early carious lesions. The pseudo-intact surface of the early enamel caries provides an ‘undisturbed compartment’ for the CRFP technology to ‘stay’ in and perform its action. Caries extending into dentin are complicated due to two factors:
REQUEST MORE INFORMATION